Iodine and Adult IQ meta-analysis
Iodine improves IQ in fetuses; adults as well? A meta-analysis of relevant studies says no.
Iodization is one of the great success stories of public health intervention: iodizing salt costs pennies per ton, but as demonstrated in randomized & natural experiments, prevents goiters, cretinism, and can boost population IQs by a fraction of a standard deviation in the most iodine-deficient populations.
These experiments are typically done on pregnant women, and results suggest that the benefits of iodization diminish throughout the trimesters of a pregnancy. So does iodization benefit normal healthy adults, potentially even ones in relatively iodine-sufficient Western countries?
Compiling existing post-natal iodization studies which use cognitive tests, I find that—outliers aside—the benefit appears to be nearly zero, and so likely it does not help normal healthy adults, particularly in Western adults.
Iodine deficiency is interesting from the ethical standpoint as one of the most cost-effective—yet obscure—public health measures ever devised which deserves a name like nootropics: a few pennies of iodine added to salt eliminates many cases of mental retardation & goiters.
Background
Supplementation of iodine in salt, water, or oil increases body iodine levels and reduces iodine deficiency disorders ( et al 2002). Supplementing, during pregnancy or infancy, can raise average IQs in the worst-off regions by <13 IQ points1 (close to a full standard deviation); such an increase is of considerable economic value, even in developed countries with iodization programs (see et al 2015 & appendices for a cost-benefit analysis). In an additional bonus for our post-feminist society, females benefit more from iodization than males2. Because salt production is generally so centralized as a bulk commodity extracted from a very few areas, iodization is almost trivial to implement. (Although humans being humans, there are obstacles even to successful iodization programs3.)
Cretinism is only the most extreme form of iodine deficiency, although a major & worthwhile humanitarian task; iodine correlates with IQ in non-deficient children, eg. Japan is simultaneously one of the longest-lived & highest IQ countries in the world and one of the greatest consumers of iodine4 (from seaweed, principally, levels so high they suggest that current recommendations are overly conservative), and even weak hypothyroidism impairs mental performance (in the old). School is directly impacted in randomized trials; from a review of Poor Economics (Banerjee & Duflo 201114ya):
Providing iodine capsules to pregnant mothers is an intervention that helps brain development in fetuses. It costs around 51 cents per dose—and leads to kids who stay in school about five months longer because they are cognitively better able to learn.
The original waves of iodization caused large-scale changes in: numbers of people going to school5, working at all6, their occupation7, how they voted, or even how many recruits from a region are accepted to selective flight schools8.
Of course, iodine can be a double-edged sword. Feyrer et al 200817ya mentioned a wave of disorders after iodization of salt, as long-deficient thyroids were shocked with adequate levels of iodine, and natural iodine levels can be so high as to begin to inversely correlate with IQ in China.9
More worrisome is recent trends in the developed world such as the War on Salt. Un-iodized salt or low-iodide salt like sea salt is ever more popular. Existing iodized table salt often has far less iodide than recommended, or even what the manufacturer claims it has10. Iodized salt used in cooking—as opposed to a straight table-side condiment—loses large chunks of its iodine content11. Small samples of ordinary people turn in severe or mild iodine deficiency rates of 67%12 to as much as 73.7%13. This is plausible given a steady secular trend of iodine reduction in the US (although one that seems to have paused in the 2000s)14. I was unsurprised to read 2012:
Numerous population studies from a variety of countries including China, Hong Kong, Iran, India, Kyrgyzstan and England have reported iodine deficiency in girls of child bearing age 76, in pregnant 154,155,156,157, and in pregnant and lactation women 158,159. Some of these studies included regions where salt iodization is practiced, yet a [substantial] proportion of pregnant and lactating women were still deficient 155,156,157,158,159,160,161. A few examples of recent studies follow…
This has led to an observable impact on the IQ of the children of English women ( et al 2013), and there is no reason to expect the effect to be confined to them.
Meta-Analysis
Given all this, one naturally wonders what the effect might be in older humans: elementary school age and above. If iodine before birth can be responsible for increasing IQ by a full standard deviation or more in combination with iron, what about iodine post-birth? Iron supplementation treats anemia and there is evidence it also treats the cognitive problems as well, so what about iodine?
Liu et al 200916ya, and tangential results like Bongers- et al 2005 (where there was a discernible IQ difference between TSH treatment of infants with congenital hypothyroidism before & after 13 days post-birth) suggest that the window for iodine intervention may close rapidly during pregnancy and be closed post-birth. While iodine has been extensively studied in infants and other unusual populations, the narrow question of iodine’s effect on IQ in healthy adult First World populations has not been (a common problem in nootropics); we are interested in cases only where someone is mentally tested before and after iodine supplementation, or where 1 cohort receives supplementation after birth when compared against a similar cohort who receive no supplementation. Most studies turn out to be either correlational (eg. stratifying by blood levels of thyroid hormone) or comparing fetal supplementation against a non-supplemented control group. Unfortunately, no study is so large and high-quality that it definitively resolves our question. So we resort to meta-analysis of what is available: we pool many studies together to derive a summary average of the overall results, weighted by how many subjects each study had (since more is better) versus how strong a result they yielded. An example of this is the meta-analysis & review, which is the closest existing study to what I want, “Iodine and Mental Development of Children 5 Years Old and Under”:
Several reviews and meta-analyses have examined the effects of iodine on mental development. None focused on young children, so they were incomplete in summarizing the effects on this important age group. The current systematic review therefore examined the relationship between iodine and mental development of children 5 years old and under. A systematic review of articles using MEDLINE (1980-November 201114ya) was carried out. We organized studies according to four designs: (1) randomized controlled trial with iodine supplementation of mothers; (2) non-randomized trial with iodine supplementation of mothers and/or infants; (3) prospective cohort study stratified by pregnant women’s iodine status; (4) prospective cohort study stratified by newborn iodine status. Average effect sizes for these four designs were 0.68 (2 RCT studies), 0.46 (8 non-RCT studies), 0.52 (9 cohort stratified by mothers’ iodine status), and 0.54 (4 cohort stratified by infants’ iodine status). This translates into 6.9 to 10.2 IQ points lower in iodine deficient children compared with iodine replete children. Thus, regardless of study design, iodine deficiency had a substantial impact on mental development. Methodological concerns included weak study designs, the omission of important confounders, small sample sizes, the lack of cluster analyses, and the lack of separate analyses of verbal and non-verbal subtests. Quantifying more precisely the contribution of iodine deficiency to delayed mental development in young children requires more well-designed randomized controlled trials, including ones on the role of iodized salt.
But its second design conflates supplementation of mothers with that of infants & children, and so the d = 0.46 (figure 2) is not directly meaningful (the authors note that the studies are heterogeneous but do not attempt stratifying by fetal vs infancy). More relevant is “Effect of iodine supplementation in pregnancy on child development and other clinical outcomes: a systematic review of randomized controlled trials”, Zhou et al 201312ya:
…Fourteen publications that involved 8 trials met the inclusion criteria. Only 2 included trials reported the growth and development of children and clinical outcomes. Iodine supplementation during pregnancy or the periconceptional period in regions of severe iodine deficiency reduced risk of cretinism, but there were no improvements in childhood intelligence, gross development, growth, or pregnancy outcomes, although there was an improvement in some motor functions. None of the remaining 6 RCTs conducted in regions of mild to moderate iodine deficiency reported childhood development or growth or pregnancy outcomes. Effects of iodine supplementation on the thyroid function of mothers and their children were inconsistent.
They correctly observe that the available studies are not very methodologically rigorous and most do not allow of any real analysis, but I think it may be worth doing a more permissive summary and see what it says. et al 2014’s “Impact of iodine supplementation in mild-to-moderate iodine deficiency: systematic review and meta-analysis” looks at Gordon & Zimmerman, combining the available tests and finding:
For the meta-analysis cognitive tests were categorised into the following domains: (i) perceptual reasoning; (ii) processing speed; (iii) working memory; and (iv) global cognitive index. The global cognitive index was derived from the average of the scores in each of the domains. Unadjusted SMDs of the change in cognitive scores from baseline were computed from the raw scores reported by the authors, while adjusted SMDs were derived from the reported mean-adjusted treatment effects. s.e.m.-adjusted treatment effects were calculated using the recommended formula in the Cochrane handbook (44). The results of the analysis for individual domains are presented in Table 3, while Fig. 3 shows the forest plots for the global cognitive index. Beneficial effects of iodine supplementation were seen for both adjusted and unadjusted global indices with mild heterogeneity observed between the studies. For individual unadjusted domain scores, benefits were seen for processing speed but not for perceptual reasoning or working memory, while for the adjusted domains iodine was beneficial for perceptual reasoning although this was associated with significant heterogeneity.
Possible Studies
I have looked at the following studies:
-
“Neurological damage to the fetus resulting from severe iodine deficiency during pregnancy”, Pharoah et al 197154ya; “The effect of iodine prophylaxis on the incidence of endemic cretinism”, Pharoah et al 197253ya; “Fetal iodine deficiency and motor performance during childhood”, Connolly et al 197946ya; “A controlled trial of iodinated oil for the prevention of endemic cretinism: a long-term follow-up”, Pharoah & Connolly 198738ya; a 196659ya Papua New Guinea trial which in 197253ya began supplementing the control group as well (who were now 0–6 years old); at the 198243ya followup, the control group still suffered cretinism and deficits compared to the experimental—no effect. These studies turn out to not test the adults or children born before iodization and so are not useful for our purpose.
-
“Prophylaxis of endemic goiter with iodized oil in rural Peru”, Pretell et al 197253ya; “Iodine deficiency and the maternal-fetal relationship”, Pretell et al 197451ya (see also the retrospective review 1994): a 196659ya Peru trial; females (<45 years old) and males (<18 years old); experimental infants did not outperform control infants—no effect. These studies turn out to not test the adults or children born before iodization and so are not useful for our purpose.
-
“The effects of oral iodized oil on intelligence, thyroid status, and somatic growth in school-age children from an area of endemic goiter”, Bautista et al. A 198243ya Bolivia trial; 200 schoolchildren measuring IQ—no effect
-
“Supplementary iodine fails to reverse hypothyroidism in adolescents and adults with endemic cretinism”, Boyages et al 199035ya; 28 Chinese aged 14–52, severely deficient, with no gains on the “Hiskey Nebraska Test of Learning Aptitude” or the “Griffiths Mental Development Scales”—no effect
-
“Controlled trial of vitamin-mineral supplementation: Effects of intelligence and performance”, Schoenthaler et al 199134ya; multivitamin with 0.075mg iodine, IQ gain in the 8th and 10th graders—beneficial effect
-
“Timing of Vulnerability of the Brain to Iodine Deficiency in Endemic Cretinism”, Cao et al 199431ya: 689 children 0–3 years of age, minimal effect in the children
-
“Dietary intake and micronutrient status of adolescents: effect of vitamin and trace element supplementation on indices of status and performance in tests of verbal and non-verbal intelligence”, Southon et al 199431ya: 13–15 year olds with a multivitamin of things including iodine (0.15mg); no effect on IQ test
-
“Effect of iodine and iron supplementation on physical, psychomotor and mental development in primary school children in Malawi” (mirror), 1994
-
“Improved iodine status is associated with improved mental performance of schoolchildren in Benin”, van den Briel et al 200025ya; originally a double-blind RCT, but subjects were contaminated by importation of iodized salt (there was an apparent small-medium effect on the matrix subtest)
-
“Cognitive and motor functions of iodine-deficient but euthyroid children in Bangladesh do not benefit from iodized poppy seed oil (Lipiodol)”, Huda et al 200124ya: 1st and 2nd grade children, ~1mg? no effect
-
“Influence of supplementary vitamins, minerals and essential fatty acids on the antisocial behavior of young adult prisoners”, Gesch et al 200223ya: over 18 prisoners, 0.14mg; beneficial effect on measures of violence, but they did not do an intelligence retest and so are not useful for our purpose.
-
“Effects of iodine supplementation during pregnancy on child growth and development at school age”, O’Donnell 200223ya; included children who were supplemented at age 2 but only tested with Raven’s at age 7, which renders their data not useful. However, the general results confirm that timing of supplementation even within pregnancy follows the ‘earlier is better’ rule.
-
“Iodine supplementation improves cognition in iodine-deficient schoolchildren in Albania”, et al 2006
-
“Effect of multivitamin and multimineral supplementation on cognitive function in men and women aged 65 years and over: a randomized controlled trial”, McNeill et al 200718ya; old adults, 0.15mg; no effect
-
“Delayed Neurobehavioral Development in Children Born to Pregnant Women with Mild Hypothyroxinemia During the First Month of Gestation: The Importance of Early Iodine Supplementation”, Berbel et al 200916ya; turns out that supplementation was administered to all women during their pregnancy, so the development scores are not useful here.
-
“Iodine supplementation improves cognition in mildly iodine-deficient children”, et al 2009
-
think2 project:
-
“The effect of iodine supplementation on cognition of mildly iodine deficient young New Zealand adults”, Fitzgerald 201213ya (see also the presentation abstract of this as et al 2012): Young adults (“18–30 years”), 33.6mg total dose; no effect. (The paper should be available in “late” 201213ya, according to Fitzgerald, but remains unavailable as of 2015-02-26.)
-
“Iodine and Cognition in Young Adults: A Randomized, Placebo-Controlled Trial” (abstract), Redman 201114ya; both Fitzgerald & Redman are reporting on the “think2” project, and the descriptions & figures reported are consistent with each other, so it seems the think2 results have been reported in separate theses.
-
-
Dewi et al 201213ya, “Iodine supplementation into drinking water improved intelligence of preschool children aged 25–59 months in Ngargoyoso sub-district, Central Java, Indonesia: A randomized control trial”; subjects selected for low urinary iodine excretion, region has >50% goiter rates
-
van Stuijvenberg et al 199926ya, “Effect of iron-, iodine-, and β-carotene -fortified biscuits on the micronutrient status of primary school children: a randomized controlled trial”
-
“Timing of the Effect of Iodine Supplementation on Intelligence Quotients of Schoolchildren”, Salarkia et al 200421ya; followup in 2 Iranian villages after the national institution of iodization in 1989
-
Untoro 199926ya, Use of Oral Iodized Oil to Control Iodine Deficiency in Indonesia, chapter 4 “Effect of stunting, iodine deficiency and oral iodized oil supplementation on cognitive performance of school children in an endemic iodine deficient area of Indonesia”, pg69–87
-
Fierro- et al 1972 & Fierro- et al 1974, which are followups to the intervention reported in Fierro- et al 1968 & et al 1969 (for a review of the Ecuadorian experiments, see 1994); a groundbreaking series of studies beginning in the 1960s in which 8 goiterous villages in Ecuador were treated with iodine injections and subsequent long-term outcomes measured through to the 1980s; for the most part, studied children were affected prenatally
-
Glinoer et al 199530ya, “A randomized trial for the treatment of mild iodine deficiency during pregnancy: maternal and neonatal effects”: pregnant women only, no cognitive measures
-
Liesenkotter et al 199629ya, “Earliest prevention of endemic goiter by iodine supplementation during pregnancy”: ditto
-
Nøhr et al 200025ya, “Postpartum thyroid dysfunction in pregnant thyroid peroxidase antibody-positive women living in an area with mild to moderate iodine deficiency: is iodine supplementation safe?”: ditto
-
Pedersen et al 199332ya, “Amelioration of some pregnancy-associated variations in thyroid function by iodine supplementation”: ditto
-
Silva & Silva 198144ya, “Interrelationships among serum thyroxine, triiodothyronine, reverse triiodothyronine, and thyroid-stimulating hormone in iodine-deficient pregnant women and their offspring: effects of iodine supplementation”: ditto
-
Mangani et al 201312ya, “Providing lipid-based nutrient supplements does not affect developmental milestones among Malawian children”: intervention included iodine (90mcg per 150g container), but the development milestones are too different from IQ or cognition to use for this
-
Santiago et al 201312ya, “Infant neurocognitive development is independent of the use of iodised salt or iodine supplements given during pregnancy”: pregnancy only
-
et al 2015, “Out of Africa: Human Capital Consequences of In Utero Conditions”: an analysis of an intriguing natural experiment, “Operation Solomon”, in which 14k Ethiopians (the entire Ethiopian Jewish community) were over 2 days airlifted from Ethiopia to Israel and settled there. Since a fair number of the women were at varying stages of pregnancy, the abruptness & comprehensiveness of the relocation means that the causal effect of better Israeli prenatal care can be inferred without any of the usual confounders which would defeat an attempt to compare Ethiopian school or test scores with Israeli. They find large effects, especially for those airlifted during the first trimester of pregnancy & for females (which is consistent with the running theme of iodine studies: that the benefits are largest when done early during pregnancy and larger for females than males). Unfortunately, it can’t be included as the design is too different, nothing similar to IQ tests were administered, and the effects reflect all the factors entailed in moving to Israel, which highly likely goes well beyond just a multivitamin.
-
et al 2015, “The Effects of Six-Month L-Thyroxine Treatment on Cognitive Functions and Event-Related Brain Potentials in Children with Subclinical Hypothyroidism”: non-randomized
-
et al 2016, “Effects of maternal and child lipid-based nutrient supplements on infant development: a randomized trial in Malawi”: randomized, and includes children 6–18mo, but assessed only on development at 18mo, which can’t be considered a useful IQ test
-
et al 2015, “Prenatal Micronutrient Supplementation Is Not Associated with Intellectual Development of Young School-Aged Children”: 3 experimental groups: folate, folate+iron, folate+iron+others+150.0mg/d iodine, allowing a comparison of folate with folate+multivitamin; but only prenatal intervention was done.
-
et al 2016, “Fortified Iodine Milk Improves Iodine Status and Cognitive Abilities in Schoolchildren Aged 7–9 Years Living in a Rural Mountainous Area of Morocco” (followup to et al 2015): relevant
-
“A cluster-randomized, controlled trial of nutritional supplementation and promotion of responsive parenting in Madagascar: the MAHAY study design and rationale”, et al 2016: preregistration of a study protocol for a Madagascar study; daily 90μg iodine in the lipid-based T2/T3 arms vs T0/T1/T4 for children aged 6–18 months, developmental outcomes “Ages and Stages Questionnaire: Inventory” & “Bayley Scale” but no IQ test-analogue.
-
“Effect of iodine supplementation during pregnancy on thyroid function and cognitive development of offspring”, Jaiswal (Bangalore India): pregnant only, no IQ tests
-
Solon et al 200322ya, “Effect of a multiple-micronutrient-fortified fruit powder beverage on the nutrition status, physical fitness, and cognitive performance of schoolchildren in the Philippines”: RCT in Philippine school-children (mean age 9.9); 4 groups total (fortified supplement x deworming), 10.8mg total iodine delivered over 16 weeks; Primary Mental Abilities Test for Filipino Children (PMAT-FC) used to measure cognitive performance
-
Lien et al 200916ya, “Impact of milk consumption on performance and health of primary school children in rural Vietnam”: claims cognitive benefits, especially to short-term memory, but paper does not report quantitative results
-
et al 2016, “Effects of pre- and post-natal lipid-based nutrient supplements on infant development in a randomized trial in Ghana” & Adu- et al 2016, “Small-quantity, lipid-based nutrient supplements provided to women during pregnancy and 6 mo postpartum and to their infants from 6 mo of age increase the mean attained length of 18-mo-old children in semi-urban Ghana: a randomized controlled trial”: measured “motor, language, socio-emotional, and executive function at 18 months” but too early for valid IQ tests, and the children appear to have received supplementation pre-natally
-
Zhou et al, “The effect of iodine supplementation in pregnancy on early childhood neurodevelopment and clinical outcomes: results of an aborted randomized placebo-controlled trial”: pregnancy only
-
2017, “Iodine Supplementation for Premature Infants Does Not Improve IQ”: Bayley-III cognitive tests at age 2, no statistically-significant difference or trend for the iodine-supplemented children (30mcg/kg/day for >3 weeks; premature infants can weigh anywhere 0.5—2.5kg) . While the supplementation is post-pregnancy, premature infants are an unusual enough patient population (and one which frequently exhibits intellectual disability or other cognitive issues) that it probably is not a good idea to meta-analyze it with RCTs on normal children & adults.
-
et al 2014/ et al 2017, “Consumption of a Double-Fortified Salt Affects Perceptual, Attentional, and Mnemonic Functioning in Women in a Randomized Controlled Trial in India”: RCT of iron+iodine supplement in 18–55yo, but where the control also received iodized salt and the large benefits were due to reducing anemia
-
“Cognitive Consequences Of Iodine Deficiency In Adolescence: Evidence From Salt Iodization In Denmark”, 2019; natural experiment using the Danish government’s legalization of and then requirement to iodize salt, 1998–3200124ya, with a difference-in-differences analysis suggesting d = 0.06 on affected adolescents’ high school GPA. (Not a RCT, and difference-in-differences are one of the weaker natural experiment designs.)
My above searches & review turned out to be partially redundant with a review that was published online a few months afterwards, in June 201213ya: Zimmerman’s “The Effects of Iodine Deficiency in Pregnancy and Infancy” and also his earlier 200916ya “Iodine deficiency in pregnancy and the effects of maternal iodine supplementation on the offspring: a review”. Regardless, the above was still useful because Zimmerman’s focus was not on any childhood or adult effects but the pregnancy & infancy effects. I have also benefited from “Iodine intake in human nutrition: a systematic literature review”. Finally, “Impact of iodine supplementation in mild-to-moderate iodine deficiency: systematic review and meta-analysis” (Taylor et al 201411ya) reviews iodine studies and for cognitive performance, meta-analyzes Gordon et al 200916ya & Zimmerman et al 200916ya, finding benefits.
Unfortunately, a few of the useful studies also tested a variety of substances, so any estimate of iodine’s effect size (such as it is) would be an overestimate: the iodine might be synergizing with one of the other ingredients (eg. iron or selenium) or the iodine might not be the responsible agent at all! We will code that covariate in. But what implications can we draw out via a meta-analysis?
Data
First, the data from the surviving studies:
|
study |
group |
year |
n.e |
mean.e |
sd.e |
n.c |
mean.c |
sd.c |
age |
dose |
multi |
country |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Bautista |
Bautista |
1982 |
100 |
69.43 |
10.96 |
100 |
70.31 |
10.96 |
8.75 |
475 |
0 |
Bolivia |
|
Boyages |
Boyages |
1990 |
28 |
34.4 |
15.4 |
24 |
29.5 |
8.5 |
29.5 |
720 |
0 |
China |
|
Schoenthaler.1 |
Schoenthaler |
1991 |
100 |
10.1 |
8.9 |
33.3 |
8.9 |
7.3 |
14 |
12.68 |
1 |
USA |
|
Schoenthaler.2 |
Schoenthaler |
1991 |
105 |
12.6 |
7.9 |
33.3 |
8.9 |
7.3 |
14 |
25.35 |
1 |
USA |
|
Schoenthaler.3 |
Schoenthaler |
1991 |
105 |
10.4 |
7.6 |
33.3 |
8.9 |
7.3 |
14 |
25.35 |
1 |
USA |
|
Southon |
Southon |
1994 |
22 |
63.94 |
2.6 |
29 |
64.1 |
1.87 |
13.5 |
16.8 |
1 |
UK |
|
Shrestha.1 |
Shrestha |
1994 |
72 |
17.1 |
1.8 |
36 |
10.7 |
2.4 |
7.1 |
490 |
0 |
Malawi |
|
Shrestha.2 |
Shrestha |
1994 |
80 |
18.2 |
1.5 |
36 |
10.7 |
2.4 |
7.1 |
490 |
0 |
Malawi |
|
Isa |
Isa |
2000 |
60 |
85.25 |
14.6 |
100 |
83.6 |
16.2 |
11.39 |
480 |
0 |
Malaysia |
|
Huda |
Huda |
2001 |
145 |
14.88 |
3.28 |
142 |
14.60 |
3.19 |
9.8 |
400 |
0 |
Bangladesh |
|
Zimmerman |
Zimmerman |
2006 |
159 |
25 |
6.3 |
151 |
20.5 |
5.6 |
11 |
400 |
0 |
Albania |
|
McNeill |
McNeill |
2007 |
398 |
11.5 |
2.3 |
374 |
11.7 |
2.1 |
72 |
54.75 |
1 |
UK |
|
Gordon |
Gordon |
2009 |
84 |
10.2 |
3 |
82 |
9.6 |
2.4 |
11.5 |
29.4 |
0 |
NZ |
|
Dewi |
Dewi |
2012 |
33 |
110.27 |
9.04 |
34 |
103.06 |
9.99 |
3.1 |
8.4 |
0 |
Indonesia |
|
Salarkia |
Salarkia |
2004 |
19 |
96 |
10 |
246 |
89 |
13 |
1.5 |
1272 |
0 |
Iran |
|
Untoro |
Untoro |
1999 |
121 |
89 |
7 |
43 |
88 |
6 |
9 |
464 |
0 |
Indonesia |
|
Redman |
Redman |
2011 |
86 |
20.85 |
3.43 |
86 |
20.59 |
3.27 |
21.28 |
45 |
0 |
NZ |
|
Solon |
Solon |
2003 |
412 |
1.82 |
0.22 |
419 |
1.66 |
0.22 |
9.9 |
10.752 |
1 |
Philippines |
Comments:
-
“age” variable is based on a simple average age in years of subjects (unweighted) or the reported mean; “dose” is total administered iodine in milligrams (note that studies typically report in micrograms/μg per day or week); multi is whether the study used solely iodine (0) or other chemicals such as iron (1)
-
Bautista notes: Stanford-Binet IQ, some data re-derived15
-
Boyages: the two groups were not randomly chosen and may have pre-existing differences in IQ
-
Schoenthaler: RAPM IQ
-
Cao: an earlier version of this meta-analysis used its “developmental quotient” excluding the pregnant women’s offspring; since this does not seem to be IQ, I removed it
-
Southon: Non-verbal IQ scores pooled16
-
McNeill: Digit span used in place of IQ scores (WM correlates highly with IQ)
-
Gordon: score from matrix subtest (1 of 4 subtest scores; 2 showed positive trend but not significance)
-
Manger: earlier version used Manger’s backwards digit span (backwards is a WM test which loads on g); however, the meta-analysis Melby-2013 & my own n-back meta-analysis found that WM exercises which transferred to digit spans did not also transfer to IQ tests, raising questions about using digit span as a proxy for IQ in a causal rather than correlational analysis
-
Stuijvenberg: see Manger
-
Isa: IQ scores reported in unhelpful format; means & deviations reverse-engineered from percentile distribution17; as usual, pregnancy-related scores are omitted
-
Shrestha: ‘Fluid intelligence’ scores reported, omitting ‘Crystallized intelligence’ & ‘Perceptual skill’; the control group is split across the iodine intervention (“Shrestha.1”) and the iodine+iron intervention (“Shrestha.2”)
-
Salarkia:
-
the paper’s original control group using contemporary age/sex-matched Tehran children, doesn’t account for their superior IQ scores and likely superior SES; I have instead used the reported 198936ya IQ scores of the previous generation of children
-
the administered iodine includes the 480mg from iodized oil but also the 6 years of iodized salt consumption (40mg/kg, national daily per capita average salt consumption 9g or 132mg a year) for a total of 1272mg
-
-
Untoro: there were 3 dose groups (200/400/800mg) but Untoro reported summary statistics for the iodine group as a whole:
The urinary iodine concentration and thyroid volume of all treatment groups were [statistically-]significantly improved after the supplementation, but there were no differences among the supplemented groups in cognitive performance. Therefore we combined the three iodized oil supplemented groups into one group.
The listed dose is a weighted average.
-
Redman: dose is calculated as: 150 μg, 100 pills a bottle, 3 bottles (1 initial bottle, 2 replacements in mail) = 150 × 100 × 3 = 45000μg; scores are from the Matrix Reasoning subtest
The result of the meta-analysis:
Random-Effects Model (k = 17; tau^2 estimator: REML)
tau^2 (estimated amount of total heterogeneity): 1.2100 (SE = 0.4432)
tau (square root of estimated tau^2 value): 1.1000
I^2 (total heterogeneity / total variability): 97.87%
H^2 (total variability / sampling variability): 47.02
Test for Heterogeneity:
Q(df = 16) = 285.8785, p-val < .0001
Model Results:
estimate se zval pval ci.lb ci.ub
0.6204 0.2716 2.2844 0.0223 0.0881 1.1527Test for Heterogeneity:
Q(df = 16) = 285.8785, p-val < .0001
Model Results:
estimate se zval pval ci.lb ci.ub
0.2565 0.0380 6.7536 <.0001 0.1820 0.3309So the effect size is, as expected, small: d = 0.2. A far cry from the d > 1 which we might estimate from the prenatal studies.
The large difference in d—0.2 vs 0.6—between the fixed-effects and random-effects models is concerning. Given the extremely high heterogeneity of the i2, which indicates that there are large differences between some of the studies, a random-effects is more appropriate in principle; but further analysis shows this is being driven by a far outlier of Shrestha, and so I believe the fixed-effects estimate of 0.2 winds up being more accurate.
A pretty forest plot summary:
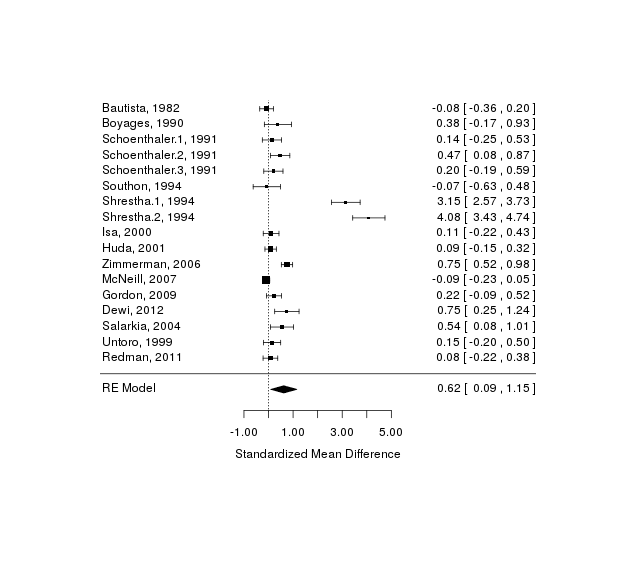
A forest plot of iodine studies
Moderators
Age & Dose
We suspected, based on the equivocal results in post-birth studies and the large decline in effect over the duration of a pregnancy in the Chinese studies, that if there was any benefit, it would be in the young; on the same reasoning, we might expect large doses to do more good than smaller ones. The necessary data is encoded into the table already, so we run a meta-analytic regression on them as independent predictors:
tau^2 (estimated amount of residual heterogeneity): 1.2521 (SE = 0.4902)
tau (square root of estimated tau^2 value): 1.1190
I^2 (residual heterogeneity / unaccounted variability): 97.49%
H^2 (unaccounted variability / sampling variability): 39.92
R^2 (amount of heterogeneity accounted for): 0.00%
Test for Residual Heterogeneity:
QE(df = 14) = 243.6469, p-val < .0001
Test of Moderators (coefficient(s) 2,3):
QM(df = 2) = 1.6083, p-val = 0.4475
Model Results:
estimate se zval pval ci.lb ci.ub
intrcpt 0.6793 0.5205 1.3053 0.1918 -0.3407 1.6994
iodine$age -0.0157 0.0183 -0.8568 0.3915 -0.0515 0.0202
iodine$dose 0.0006 0.0009 0.6665 0.5051 -0.0011 0.0023The coefficients and variability are disappointing: the age and dose moderators explain little of what is going on.
Some graphs to help us visualize. Graphing by age, we see what might be a slight negative relationship, as the regression suggests (driven by Shrestha 199431ya):
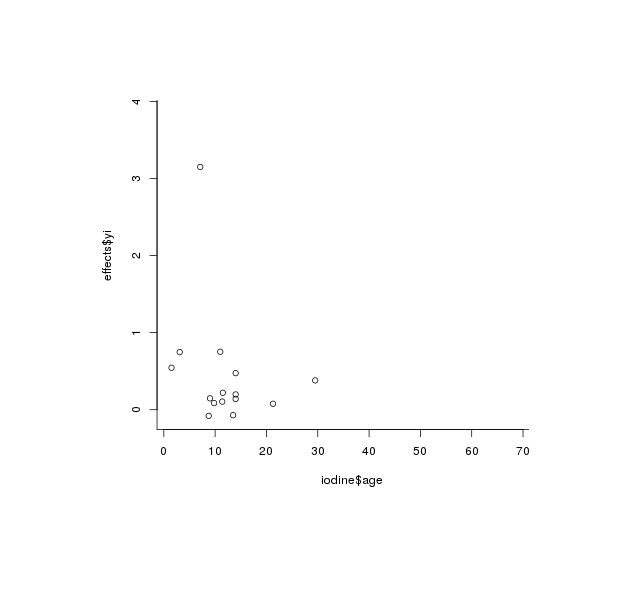
plot(iodine$age, effects$yi)
Graphing by dose, we see—despite the calculated statistical-significance—no relationship at all to my eyes (outliers are Shrestha 199431ya, again):
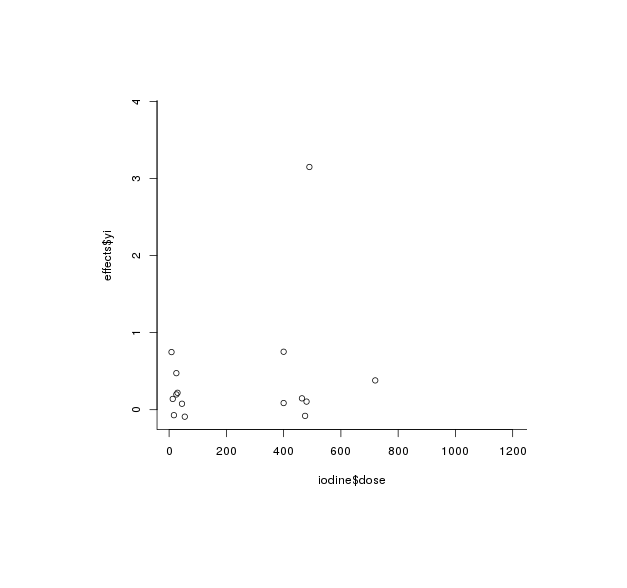
plot(iodine$dose, effects$yi)
The estimate is the important part: neither of the moderators seem to have a strong relationship with the cognitive benefits (nor are they at least statistically-significant). It would seem that any effectiveness of iodine is unrelated to age and dose. Whether the effectiveness is being driven by a few studies is what we’ll look at next.
Multiple Supplements
One methodological concern is that by including studies like Southon which supplemented many things besides iodine, our results are merely picking up the efficacy of other supplements (iron is a particular concern). Curiously, despite our expectation that the multi-vitamin studies would have higher effect sizes because any of the ingredients could be helpful singly or synergistically, it is strikingly the opposite:
QM(df = 2) = 6.7027, p-val = 0.0350
Model Results:
estimate se zval pval ci.lb ci.ub
factor(iodine$multi)0 0.8250 0.3203 2.5756 0.0100 0.1972 1.4529
factor(iodine$multi)1 0.1300 0.4953 0.2625 0.7930 -0.8408 1.1008Bias Checks
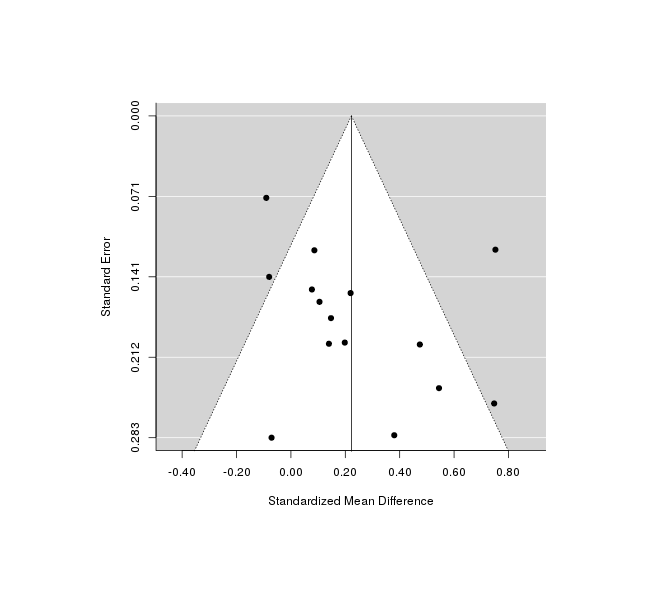
We do not have enough to reliably check for biases like publication bias, but we can still try. The funnel plot looks pretty bizarre, with almost all studies tightly bunched around the null effect but 2 outliers—the 2 Shrestha 199431ya groups we just saw—showing shockingly high effect sizes of d = 3.1/4.1. Why did Shrestha 199431ya observe such large IQ effects? I don’t know, although the Malawi region was chosen for its iodine deficiency.
A test & graph:
test for funnel plot asymmetry: z = 3.3206, p = 0.0009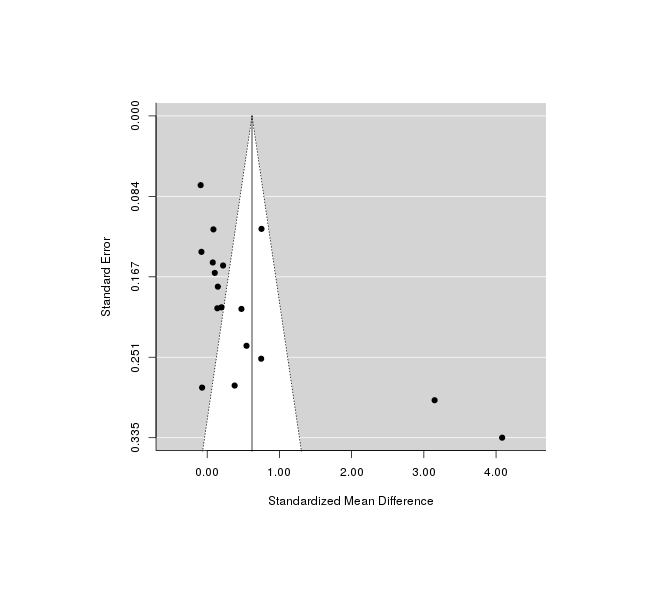
A funnel plot of effect size versus sample size, checking for bias in publishing only good-looking results on iodine
So Shrestha 199431ya is driving most of the effect! (Not a surprise at this point.) If we omit those points, the funnel plot is cleaner
A funnel plot with Shrestha removed, showing better fit from the weaker estimate.
A trim-and-fill check agrees with us and not the test, by deciding not to add in any new studies between Shrestha and the rest; we also notice that the τ2 & i2 are extremely high, which is just telling us what we know—Shrestha 199431ya is different from the other studies:
Estimated number of missing studies on the left side: 0 (SE = NA)
Random-Effects Model (k = 17; tau^2 estimator: REML)
tau^2 (estimated amount of total heterogeneity): 1.2100 (SE = 0.4432)
tau (square root of estimated tau^2 value): 1.1000
I^2 (total heterogeneity / total variability): 97.87%
H^2 (total variability / sampling variability): 47.02If we were to redo the analysis but omitting Shrestha 199431ya, we see a much smaller effect-size:
Random-Effects Model (k = 15; tau^2 estimator: REML)
tau^2 (estimated amount of total heterogeneity): 0.0526 (SE = 0.0313)
tau (square root of estimated tau^2 value): 0.2293
I^2 (total heterogeneity / total variability): 68.75%
H^2 (total variability / sampling variability): 3.20
Test for Heterogeneity:
Q(df = 14) = 53.0253, p-val < .0001
Model Results:
estimate se zval pval ci.lb ci.ub
0.2224 0.0751 2.9602 0.0031 0.0752 0.3697So, it seems a lot of the effect size is being driven by a few studies turning in large or extremely large effect sizes: Shrestha, Zimmerman, and Dewi (in chronological order). One common factor to these studies seems to be that they worked in the most iodine-deprived areas possible: Shrestha chose his region as being the worst he could find, and Dewi cites reports of goiter in half the population while targeting the supplementation to the most deficient children.
At most, we can justify an effect estimate which is much smaller than would be estimated based on the prenatal studies, and the reality of this residual effect can be doubted: looking at the forest plot, the more rigorous and Western studies seem to have the tiniest and closest to zero estimates.
Code
Run as R --slave --file=iodine.r:
set.seed(7777) # for reproducible numbers
# TODO: factor out common parts of `png` (& make less square), and `rma` calls
# install.packages("XML") # if not installed
library(XML)
iodine <- readHTMLTable(colClasses = c("character", "integer", rep("numeric", 8)),
"https://gwern.net#data")[[1]]
# install.packages("metafor") # if not installed
library(metafor)
effects <- escalc("SMD", m1i = mean.e, m2i = mean.c, sd1i = sd.e, sd2i = sd.c, n1i = n.e, n2i = n.c,
data = iodine)
cat("Basic random-effects meta-analysis of all studies:\n")
res1 <- rma(yi, vi, data = effects); res1
cat("Fixed-effects version:\n")
res2 <- rma(yi, vi, data = effects, method="FE"); res2
png(file="~/wiki/doc/iodine/gwern-iodization-forest.png", width = 480, height = 480)
forest(res1, slab = paste(iodine$study, iodine$year, sep = ", "))
invisible(dev.off())
cat("Random-effects with age & dose moderators:\n")
rma(yi, vi, mods = ~ iodine$age + iodine$dose, data = effects)
png(file="~/wiki/doc/iodine/gwern-age.png", width = 480, height = 480)
plot(iodine$age, effects$yi)
invisible(dev.off())
png(file="~/wiki/doc/iodine/gwern-dose.png", width = 480, height = 480)
plot(iodine$dose, effects$yi)
invisible(dev.off())
cat("Check random-effects meta-analysis for whether the multiple-supplement trials are inflating results:\n")
rma(yi, vi, mods = ~ factor(iodine$multi) - 1, data = effects)
png(file="~/wiki/doc/iodine/gwern-iodization-funnel.png", width = 480, height = 480)
funnel(res1)
invisible(dev.off())
cat("The funnel plot looks weird, test it:\n")
regtest(res1, model = "rma", predictor = "sei", ni = NULL)
cat("For kicks, what does a (normal) trim-and-fill say?\n")
tf <- trimfill(res1); tf
cat("Re-run random-effects meta-analysis, omitting Shrestha:\n")
res3 <- rma(yi, vi, data = escalc("SMD", m1i = mean.e, m2i = mean.c, sd1i = sd.e, sd2i = sd.c,
n1i = n.e, n2i = n.c,
data = iodine[!(grepl("Shrestha", iodine$study)),])); res3
# funnel plot with Shrestha omitted
png(file="~/wiki/doc/iodine/gwern-funnel-moderated.png", width = 480, height = 480)
funnel(res3)
invisible(dev.off())
# optimize the generated graphs by cropping whitespace & losslessly compressing them
system(paste('cd ~/wiki/image/iodine/ &&',
'for f in *.png; do convert "$f" -crop',
'`nice convert "$f" -virtual-pixel edge -blur 0x5 -fuzz 10% -trim -format',
'\'%wx%h%O\' info:` +repage "$f"; done'))
system("optipng -o9 -fix ~/wiki/image/iodine/*.png", ignore.stdout = TRUE)See Also
-
Iodine section of Nootropics essay -(motivation; some statistical power calculations for a self-experiment looking for cognitive improvement; a “value of information” calculation on the possible benefit versus the quality of information from self-experimenting; a silly eye-color experiment resulting in no change from supplementation)
-
See Scrimshaw 199827ya; Bleichrodt & Born 199431ya; and et al 2005:
↩︎Thirty-seven reported studies, total 12,291 children, were analysed. The effect size was an increase of 0.83, 0.82, and 0.32 SIQP respectively, for the children living in IS communities compared with those living in ID areas with no iodine supplementation, with inadequate iodine supplementation, or children who had received iodine during their mothers’ pregnancy and after birth. These equal to 12.45, 12.3, 4.8 IQ points. Compared with that of children whose mothers were persistently exposed to ID, the total effect size of the 21 entries was an increase of 0.58 SIQP (8.7 IQ points) in the group receiving iodine supplementation during pregnancy. Furthermore, there was an increase on 1.15 SIQP of Binet or 0.8 SIQP on Raven Scale (17.25 or 12 IQ points) for children born more than 3.5 years after iodine supplementation program was introduced. The level of iodine nutrition plays a crucial role in the intellectual development of children. The intelligence damage of children exposed to severe ID was profound, demonstrated by 12.45 IQ points loss and they recovered 8.7 IQ points with iodine supplementation or IS before and during pregnancy
-
“IQ in the Ramsey Model: A Naïve Calibration”, Jones 200619ya:
In a recently published paper, Erica Field, Omar Robles, and Maximo Torero study the effects of iodine deficiency on educational attainment in Tanzania (Field, Robles and 2009). Theirs is the first published paper to link economically [important] outcomes to iodine deficiency, and it supports the idea of improved schooling outcomes after iodine supplementation. Interestingly, Field et al. also find bigger effects for females, which could be due either to biological differences or differences associated with intra-household resource allocation and social responses to increased cognition of males and females.
The original:
↩︎Our findings suggest that reducing fetal IDD has [substantial] benefits for child cognition: Children who receive iodine in utero attain an average of 0.33 years of education above siblings and older and younger children in their district. Furthermore, the effects appear to be substantially larger for girls, consistent with new evidence from laboratory studies in animals indicating greater cognitive sensitivity of the female fetus to in utero iodine deprivation, including sex-specific responses to maternal thyroid hormone restriction on expression of neural thyroid hormone receptors. The results are consistent across household and district fixed effects models and patterns of variation in estimated effects are consistent with predictions regarding the vulnerability of specific subpopulations to fetal IDD. Cross-country regression estimates indicate a strong negative influence of total goiter rate and strong positive influence of salt iodization on female school participation.
-
An example of the commercial opposition or conspiracy theorists is the Kazakhstan campaign; from “In Raising the World’s I.Q., the Secret’s in the Salt”, NYT:
↩︎In fact, Kazakhstan has become an example of how even a vast and still-developing nation like this Central Asian country can achieve a remarkable public health success. In 199926ya, only 29% of its households were using iodized salt. Now, 94% are. Next year, the United Nations is expected to certify it officially free of iodine deficiency disorders…Largely out of the public eye, they made terrific progress: 25% of the world’s households consumed iodized salt in 199035ya. Now, about 66% do.
…In some nations, iodization becomes tarred as a government plot to poison an essential of life—salt experts compare it to the furious opposition by 1950s conservatives to fluoridation of American water. In others, civil libertarians demand a right to choose plain salt, with the result that the iodized kind rarely reaches the poor. Small salt makers who fear extra expense often lobby against it. So do makers of iodine pills who fear losing their market. Rumors inevitably swirl: iodine has been blamed for AIDS, diabetes, seizures, impotence and peevishness. Iodized salt, according to different national rumor mills, will make pickled vegetables explode, ruin caviar or soften hard cheese. Breaking down that resistance takes both money and leadership…The country’s biggest salt company was initially reluctant to cooperate, fearing higher costs, a Unicef report said. Cardiologists argued against iodization, fearing it would encourage people to use more salt, which can raise blood pressure. More insidious, Dr. Sharmanov said, were private companies that sold iodine pills. “They promoted their products in the mass media, saying iodized salt was dangerous,” he said, shaking his head…Asked about the Unicef report saying that Aral Tuz initially resisted iodization on the grounds that it would eat up 7% of profits, the company’s president, Ontalap Akhmetov, seemed puzzled. “I’ve only been president three years,” he said. “But that makes no sense.” The expense, he said, was minimal. “Only a few cents a ton.”
…In the 1990s, when the campaign for iodization began, the world’s greatest concentration of iodine-deficient countries was in the landlocked former Soviet republics of Central Asia. All of them—Kazakhstan, Turkmenistan, Tajikistan, Uzbekistan, Kyrgyzstan—saw their economies break down with the collapse of the Soviet Union. Across the region, only 28% of all households used iodized salt. “With the collapse of the system, certain babies went out with the bathwater, and iodization was one of them,” said Alexandre Zouev, chief Unicef representative in Kazakhstan…That combination is missing in many nations where iodine deficiency remains a health crisis. In nearby Pakistan, for instance, where 70% of households have no iodized salt, there are more than 600 small salt producers. [see “Pakistan takes legal action”, Unicef; for further reading, the WHO’s Assessment of iodine deficiency disorders and monitoring their elimination]
-
average daily Japanese consumption of iodine ranges from 5.28-13.8mg of iodine; Patrick L. Iodine: deficiency and therapeutic considerations, although Gaby argues this is a misinterpretation: “the idea that Japanese people consume 13.8 mg of iodine per day appears to have arisen from a misinterpretation of a paper. In that paper, the average intake of seaweed in Japan was listed as 4.6 g (4,600 mg) per day, and seaweed was said to contain 0.3% iodine. The figure of 13.8 mg comes from multiplying 4,600 mg by 0.003. However, the 4.6 g of seaweed consumed per day was expressed as wet weight, whereas the 0.3%-iodine figure based on dry weight. Since many vegetables contain at least 90% water, 13.8 mg per day is a [large] overestimate of iodine intake. In studies that have specifically looked at iodine intake among Japanese people, the mean dietary intake (estimated from urinary iodine excretion) was in the range of 330 to 500 mcg per day, which is at least 2.5-fold lower than 13.8 mg per day.” Abraham replies “The urinary excretions of iodide reported by Ishizuki et al in references 7 and 8 of Gaby’s editorial are obviously from patients who were told to abstain from seaweed. We will quote other studies by Japanese investigators who reported urinary iodide levels 10 to 100 time higher than the values reported by Ishizuki et al .”↩︎
-
“The Impact of Iodine Deficiency Eradication on Schooling: Evidence from the Introduction of Iodized Salt in Switzerland”, Politi 201411ya (see also Field et al 200916ya):
↩︎I identify the impact of iodization in three ways: first, in a differences-in-differences framework, I exploit geographic variation in iodine deficiency, as well as the fact that the nationwide campaign to decrease iodine deficiency began in 1922103ya. Second, I use spatial and temporal variation in the introduction of iodized salt across Swiss cantons, and examine whether the level of iodized salt sales at the time of one’s birth affected one’s educational attainment. Third, I employ a fuzzy regression discontinuity design and use jumps in sales of iodized salt across Swiss cantons to identify the effect of iodization, by comparing outcomes for those born right before and right after these sudden changes in the treatment environment. These approaches indicate that the eradication of iodine deficiency in previously deficient areas increased the schooling of the population [statistically-]significantly. The effects are larger for females than for males, which is consistent with medical evidence showing that women are more likely to be affected by iodine deficiency disorders than men.
-
“Salt Iodization and the Enfranchisement of the American Worker”, Adhvaryu et al 201312ya:
↩︎…We find substantial impacts of salt iodization. High school completion rose by 6 percentage points, and labor force participation went up by 1 point. Analysis of income transitions by quantile shows that the new labor force joiners entered at the bottom of the wage distribution and took up blue collar labor, pulling down average wage income conditional on employment. Our results inform the ongoing debate on salt iodization in many low-income countries. We show that large-scale iodized salt distribution had a targeted impact, benefiting the worker on the margin of employment, and generating sizeable economic returns at low cost.
-
2015, “The effects of the generalized use of iodized salt on occupational patterns in Switzerland”↩︎
-
“The Economic Effects of Micronutrient Deficiency: Evidence from Salt Iodization in the United States”, Feyrer et al 200817ya (quotes are from 200817ya draft, not 2013 final version):
For instance, Sachs (200322ya) shows that efforts to eliminate malaria have substantial effects on income, through their effect on health, reduced absenteeism, etc. 2007 look at the effect of health interventions and find little effect. Weil (200718ya) charts a middle course…For example, Bleakley (200718ya) examines the effects of hookworm eradication in the American South in early 20th century and finds [substantial] effects on education and future incomes of those cohorts that benefited from the intervention.
-
Bleakley, Hoyt, “Disease and Development: Evidence from Hookworm Eradication in the American South”, Quarterly Journal of Economics, February 200718ya, 122 (1), 73–117 [but see Roodman’s contrary analysis, “Questioning the evidence on hookworm eradication in the American South”, based on analyzing the de-aggregated data.]
…Figure 1 illustrates the geographic distribution of goiter in the US as measured among World War I recruits (we discuss the data further below). In 1924101ya iodized salt was introduced in the United States explicitly to reduce the goiter rate. This intervention rapidly reduced the incidence of iodine deficiency. Iodization of salt in the US provides a particularly good natural experiment due to the geographic distribution of the disease combined with a rapid, complete treatment. Since there are large in utero effects of iodine deficiency, we should see a [substantial] difference between those born before and after the introduction of iodized salt in locations with low levels of environmental iodine. Those living in high iodine regions provide a control group…The probability of assignment to the Air Corps rises [substantially] in low iodine (ie. high goiter) counties in the years after the introduction of iodized salt. In the lowest iodine regions, our estimates suggest a 10–20% increase in the probability of a man being assigned to the Air Corps after iodization. Using information about average scores of Air and Ground Force recruits we can infer a one-quarter to one half standard deviation increase in average test scores in these regions. The average level of iodine deficiency in the US was [substantially] lower than in the highest regions, so the overall effect in the US was much more modest, though iodization was undoubtedly extremely cost effective. The increase in cognitive ability due to salt iodization may have contributed a small amount to trend rise in measured IQ that took place over the course of the twentieth century, the so-called Flynn Effect…2004 find that differences in birth weight among identical twins are reflected in differences in school attainment and adult earnings…More cites to be added, including Case & Paxson.
Typically, non-deficient populations differ from iodine-deficient populations by approximately 10 IQ points, whereas the whole normal IQ distribution of a population shifts to the left as a result of iodine deficiency7. In endemic areas, cretinism can affect up to 15% of the population (de Benoist et al eds 200421ya). Bleichrodt & Born 199431ya estimate that the average IQ of iodine-deficient groups is 13.5 points lower than the non-deficient groups…Scrimshaw (199827ya) provides a list of studies and experiments that have been conducted, and which have shown the hindering effects on mental development of iodine deficiency in utero.
-
7: Scrimshaw (199827ya) provides a list of studies and experiments that have been conducted, and which have shown the hindering effects on mental development of iodine deficiency in utero.
-
de Benoist, Bruno, Maria Andersson, Ines Egli, Bahi Takkouche, and Henrietta Allen, eds, Iodine status worldwide: WHO Global Database on Iodine Deficiency, Geneva, Switzerland: World Health Organization, 2004
-
Bleichrodt, N and M P Born, “A meta-analysis of research on iodine and its relationship to cognitive development,” in John B. Stanbury, ed., The damaged brain of iodine deficiency, New York: Cognizant Communication, 199431ya, pp. 195–200
…It had been documented that large amounts of iodine could cause hyperthyroidism to develop in some adults and thyrotoxicosis in others…thyrotoxicosis might occur as a result of iodization in those individuals that have suffered from long-term iodine deficiency and whose goiters have become nodular. In such cases, iodine supplementation causes the output of hormone to jump to toxic levels…The number of enlisted men started increasing in 194283ya, and it peaked in the second semester of that year, as well as the first semester of 194382ya. People born after iodization enlisted in large numbers starting the first semester of 194382ya. The proportion of recruits going to the Air Force was particularly low in 194382ya…How large are these effects? The highest goiter places have goiter rates of 30. The coefficients (from Table 4) suggest that about 15% more recruits from the highest goiter regions go into the AAF after salt iodization. From Appendix A we know that the Air Force recruits have, on average 9 point higher AGCT scores (almost a half a standard deviation). The average increase for the recruits from that section is therefore 0.15 time 9 points, or 1.35. So the average cognitive ability in the section goes up by greater than one twentieth of a standard deviation. Examining the high-low regressions yields similar figures. In the high goiter group, we have a 5–10% higher assignment rate to the AAF after salt iodization. 10% times 8 AGCT points results in 0.8 points higher on average, or about a twentieth of a standard deviation. This implies a twentieth of a standard deviation increase in cognitive ability for 25% of the US population.
The final version finds a more substantial effect:
The estimated coefficient on the high-goiter dummy in table 5 is in the range 2.5–8.7 percentage points. Similarly, the logit specification in Table 8 implies a marginal effect of iodization on the probability of entering the AAF in the range of 3–7.8 percentage points. Comparing these estimates to Table 9, we see that the lower range of these estimates are consistent with iodization raising IQ by 15 points (that is, X = 15), which is a reasonable expectation given the work of (Bleichrodt and Born 199431ya). However, the higher range of estimates is larger than any reasonable estimate of the increase in IQ that would have resulted from iodization. Given the uncertainty surrounding the selection process and prior literature on iodization we do not consider the larger results plausible. In any case, our results are consistent with a substantial effect in line with the existing literature.
But unfortunately, the detailed mechanisms & psychometrics are insufficient to support a concrete estimate of IQ gains, as taken literally, their results indicate an IQ gain somewhere around 30 points; this is sufficiently large as to prove that the analysis is not fully capturing the dynamics and the estimates cannot be taken literally aside from proving that there was probably a substantial gain. (Based on the many problems with the iodization literature, suggesting 15 points is probably an overestimate.)
Another interesting paper exploits the similarly abrupt introduction of iron fortification into the USA ~WWII: “Ironing Out Deficiencies: Evidence from the United States on the Economic Effects of Iron Deficiency”, 2015.↩︎
-
-
“Effects of drinking water with high iodine concentration on the intelligence of children in Tianjin, China” (slides), Liu et al 200916ya:
↩︎The results indicated that for children who resided in regions with a very high water iodine concentration, there was on average a reduction of IQ by nearly nine points (b = −8.7, 95% CI: −15.9 to −1.4) in comparison with those who resided in a non-high water iodine area. When comparing children living in areas with a high water iodine concentration with those in the non-high areas, a slight reduction of IQ by about two points was observed, however, it was not [statistically-]significant. There was also a [statistically-]significant association between year of birth and IQ, which seemed to exhibit a dose-response relationship. There was a progressive increase in IQ by about four (p = 0.072) and eight (p = 0.015) points for children born in 199629ya and 199728ya when compared with those who were born in 199530ya, the year China first implemented the national dietary iodine supplement programme.
-
Analyzed 88 samples; 47 fell below USFDA recommended level and their labeled level: Dasgupta PK, Liu Y, Dyke JV. “Iodine nutrition: iodine content of iodized salt in the United States”↩︎
-
Salt in cooking meat loses ~60% of iodine; Wang et al 199926ya, Effects of storage and cooking on the iodine content in iodized salt and study on monitoring iodine content in iodized salt↩︎
-
“Iodine status of UK schoolgirls: a cross-sectional survey”, Vanderpump et al 201114ya; see also “The prevalence of iodine deficiency in women of reproductive age in the United States of America”, et al 2007↩︎
-
Gunton JE, Hams G, Fiegert M, McElduff A. Iodine deficiency in ambulatory participants at a Sydney teaching hospital: is Australia truly iodine replete?; see also et al 2013.↩︎
-
Hoption Cann SA. “Hypothesis: dietary iodine intake in the etiology of cardiovascular disease”:
In the general United States (US) population, a declining trend in urinary iodine levels has been observed as estimated through the large National Health and Nutrition Examination Surveys (NHANES I, 1971–74; and NHANES III, 1988–94) [3]. The proportion of the US population with moderate to severe iodine deficiency (<50 μg iodine/L in urine) has more than quadrupled in the last 20 years, 2.6% in NHANES I vs 11.7% in NHANES III [3]. This decline may be due to a reduced intake of iodized salt. For example, Enstrom et al. [4] compared data from nationally representative samples of the American population from two time periods, 1980–2198243ya vs 1990–2199233ya. Based on dietary intake studies from over 10,000 individuals, no change was observed in sodium intake from food, while there was a 65% decline in sodium intake from discretionary (iodized) salt. Adventitious sources of iodine have also declined with reductions in the use of iodine in the dairy industry and in commercial bread production [5]. Comparable trends have been observed in other countries that iodize salt. For example, public health recommendations to reduce salt intake have been implicated in the decreasing iodine status in Australia and New Zealand [6]. Similarly, a recent decline in median urinary iodine levels in Austria may be due to lower salt intake as well as the availability of noniodized salt in Austria after joining the European Union in 199530ya [7]. In Greenland, as imported foods have replaced consumption of traditional foods such as fish and sea mammals, there has been a gradual decline in iodine status. Andersen et al. [8] found that median urinary iodine excretion declined with the degree of decrease in the traditional lifestyle. Evidence of iodine deficiency was seen in non-Inuit subjects, who had the lowest levels. Thus, in countries where there are changing dietary patterns, including those long established iodization programs, [substantial] declines in iodine intake may occur.
See also et al 2005; et al 2004; et al 2013; and et al 2013↩︎
-
Bautista did not report standard deviations, but did report ns, means, and p-values, which permits the standard deviation to be derived, following the Cochrane Handbook (“7.7.3.3 Obtaining standard deviations from standard errors, confidence intervals, t values and p values for differences in means”): the degrees of freedom = 198, so with a reported p = 0.57, t = 0.569; then the standard error is the means divided by the t value ((70.31 − 69.43) / 0.569); and finally the standard deviation: 1.55 / √(1⁄100 + 1⁄100) = 10.96.↩︎
-
Southon reported control & experimental scores split by gender, which need to be re-pooled:
-
control
-
n = 9 + 20 = 29
-
mean = ((60.6 × 9) + (65.6 × 20)) / (9 + 20) = 64.1
-
standard deviation = (((9 − 1) × 2.3) + ((20 − 1) × 1.7)) / (9 + 20 − 2) = 1.87
-
-
active
-
n = 10 + 12 = 22
-
mean = ((10 × 63.4) + (12 × 64.4)) / (10 + 12) = 63.94
-
standard deviation = (((10 − 1) × 2.6) + ((12 − 1) × 2.6)) / (10 + 12 − 2) = 2.6
-
-
-
See Table 7; 12 month followup scores are reported grouped in IQ deciles, and if one assumes scores in each decile average to around the median (since they should be following a bell curve, this will overstate standard deviations), one can calculate out the figures in R as follows:
↩︎# experimental sd(c(rep(65,12), rep(75,10), rep(85,17), rep(100,19), rep(115,1), rep(125,1), rep(135,0))) [1] 14.59699 mean(c(rep(65,12), rep(75,10), rep(85,17), rep(100,19), rep(115,1), rep(125,1), rep(135,0))) [1] 85.25 # control sd(c(rep(65,30), rep(75,13), rep(85,25), rep(100,26), rep(115,5), rep(125,0), rep(135,1))) [1] 16.19141 mean(c(rep(65,30), rep(75,13), rep(85,25), rep(100,26), rep(115,5), rep(125,0), rep(135,1))) [1] 83.6